
More HIV Prevention Options: An AIDS 2020 Update
During the AIDS 2020 virtual conference, the promising results from the HPTN 083 trial of long acting injectable cabotegravir for PrEP among men who have sex with men and transgender women were presented. News headlines and HIV prevention advocates hailed the promise of a new HIV prevention method to add to the HIV prevention “toolkit”. Interested in learning more? AVAC has created a primer for advocates on long acting injectable cabotegravir for PrEP. A week after AIDS 2020, the vaginal ring for HIV prevention was in the news as the European Medicines Agency (EMA) adopted a positive scientific opinion about the use of the dapivirine vaginal ring for use by cisgender women ages 18 and older in developing countries.
Let’s put this good news in context. What have we learned from eight years of PrEP implementation in the U.S., since the July 2012 FDA approval of daily oral TDF/FTC for PrEP? What have we learned from implementation of injectable forms of birth control? During a non-AIDS 2020 webinar I attended during the conference week, Policing without the Police: Race, Technology, and the New Jim Crow, Drs. Benjamin and Roberts discuss racial inequity and technology. “Emerging biomedical technologies always widen disparities,” they shared. This disparity has been true in uptake of the daily HIV prevention pill. How might this knowledge inform our next generation of PrEP implementation to inform the development of best practices to achieve equitable decreases in HIV diagnosis and equitable increases in sexual empowerment among people who could benefit from PrEP in the U.S.?
In this blog, I share my sketchnotes and insights from attending AIDS 2020 (thank you to the AIDS 2020 Local Planning Group for the scholarship!). If you are interested in other highlights from AIDS 2020, check out this New England Journal of Medicine (NEJM) “Really Rapid Review” for more good news. I’m eager for a dialogue on how we can do more, how we can do better. Let’s go!
Beyond Daily PrEP: Dr. Susan Buchbinder provides context for where to place the promise of new HIV prevention methods within the larger landscape.
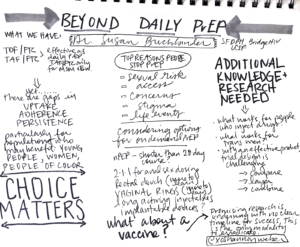
Grounding us with what we currently know, Dr. Buchbinder reminds us we have one highly effective prevention method (daily TDF/FTC) and a second highly effective method (TAF/FTC) for gay and bi cisgender men. Yet, there are gaps across the PrEP or HIV prevention continuum in uptake, adherence, and persistence (which can also be thought of as retention in care) particularly for people of color, young people, and women. Among the top reasons people stop PrEP include: their real or perceived sexual risk has changed, access issues, concerns, stigma, and life events. Choice in options matters; as a lesson learned from family planning an increase in options expands uptake overall. What options might we consider? On demand or event based PrEP has been adopted at the same gender loving men at the community level in the U.S. after successful study data from Canada and Europe was published. On demand or event based PrEP has not been approved by the CDC, which slows uptake at the systems level of this method in the U.S. There is promising data from HIV prevention trials including rectal douches, vaginal rings, long acting injectables, as well as implantable devices. With a known effective HIV prevention method (the daily pill), there are design challenges in developing the needed new research for both the primary efficacy data as well as implementation. Experts are developing ethical methods for rolling out the needed clinical trials and implementation studies in priority populations and with promising methods. In lieu of a “silver bullet” in HIV prevention, what about a vaccine? Promising research is underway though there is no clear timeline for success. In short, there are more options on the horizon though, none of these new methods alone solve the current bleak gaps in uptake, adherence and persistence.
Dr. Dominka Seidman shares lessons learned from injectable contraception.
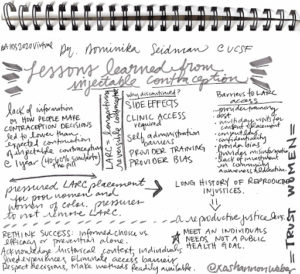
Lessons learned from implementation of injectable contraception may inform rollout of injectable HIV prevention methods. Importantly, lack of information on how people make contraceptive decisions led to lower than expected continuation of injectable contraception at one year. Poor women and women of color were pressured to choose long acting reversible contraceptives (LARC); additionally there were pressures to not remove LARC or support of women’s decision making. Not dissimilar to PrEP implementation, barriers to LARC access include: providing training, cost, multi-day visits for consent and placement, consent laws, confidentiality, provider bias, provider misinformation, and lack of investment in community awareness and education. Within the family planning field they have learned to rethink success balancing informed choice versus efficacy or prevention alone. It is important to acknowledge the historical context of racism as well as individuals’ lived experiences as we eliminate access barriers. Finally, respect people’s decisions and make the menu of prevention options readily available.
Dr. Al Liu presents person centered care as the cornerstone in his talk “PrEP with the people.”
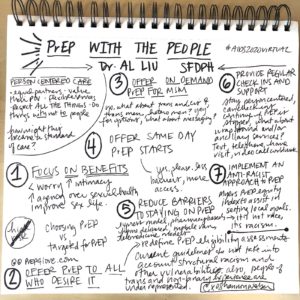
Al Liu shares insights on how person centered care and working with not for people can enhance PrEP uptake. Based in the principles of person centered care where patients are seen as equal partners in the decision making process and their point of view is valued, Al provides seven tips for scaling person centered PrEP services.
1) Focus on benefits
2) Offer PrEP to all who desire it
3) Offer on demand PrEP for MSM
4) Offer same day PrEP starts
5) Reduce barriers to staying on PrEP
6) Provide check ins and support
7) Implement an anti-racist approach to PrEP
Realizing the promise of HIV prevention is more than focusing solely on the pill or medication. Rather, we need to confront structural racism, the siloed systems that perpetuate inequities and remember there is no pill or medication without access the ancillary services to support person-centered care and decision making from a harm reduction approach.
